Surname/Family name of individual being assessed for NHS CHC
Required
First name/s
Required
NHS number
Other identifier (please specify) if NHS number not known
Permanent address
Required
Telephone number
Required
Responsible Professional Name *
Required
Job title
Required
Organisation
Required
Email address for responsible professional
Required
Telephone number for responsible professional
Required
* All relevant sections to be completed by the responsible professional. In this context the ‘responsible professional’ means the professional who is responsible for obtaining consent to share with third parties, normally at Checklist stage. Since the Checklist can be completed by a range of professionals any of these could be the ‘responsible professional’ in terms of gaining consent for sharing information with Family, Friends and Representatives
Describe what steps have been taken to enable the person to make the informed decision themselves:(e.g. interpreter, communication aids, relevant information in an accessible form, consider time of day when their ability to understand is better, treating a medical condition which may be affecting their mental capacity, involving someone who knows them etc .)
If yes, how have these been addressed?
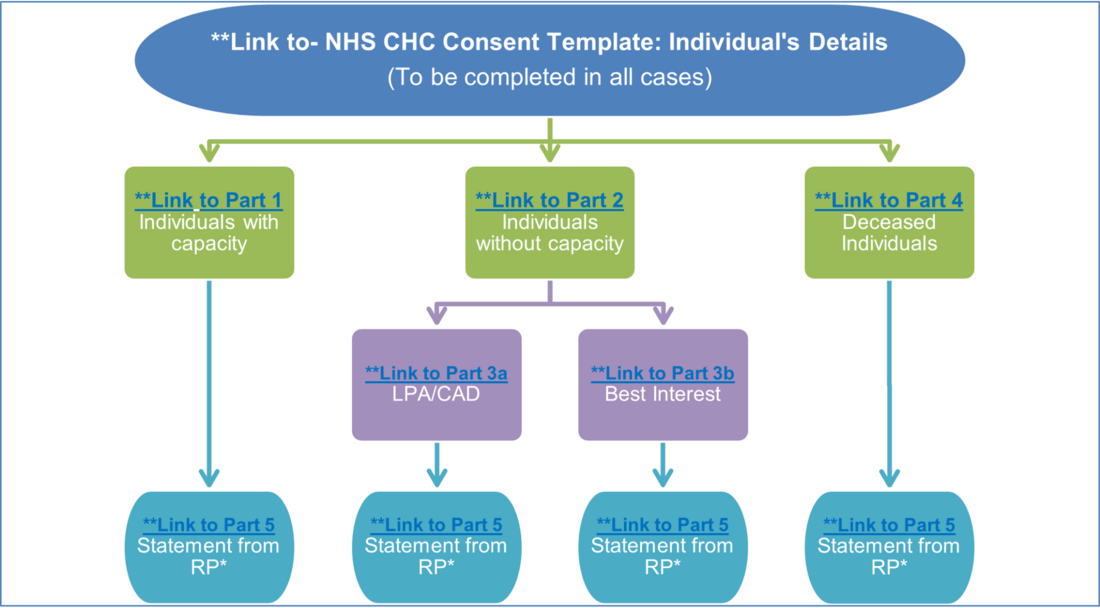
Part 1 – Consent from Individuals Who Have Capacity.
Statement of consent to share information with Family, Friends and Representatives (Please refer to Part 5)
Provide details of who the individual has consented to access their health and care information. Name/ Relationship/ Address and telephone number/ Notes (for example request for a specific piece of information to be withheld)
Full name entered below will serve as my electronic signature, confirming that the information provided is accurate to the best of my knowledge.
Part 2 - Where the Responsible Professional has reason to believe that the Individual may lack capacity to consent for Information Sharing with Family, Friends, and Representatives
Mental Capacity Assessment / Record of Determination:
In relation to the decision whether or not to share personal health and social care information with family/friends/representatives for the purpose of assessing eligibility for NHS Continuing Healthcare:
a. At the date and time of this assessment, is the person able to understand the information relevant to the decision?
** None Yes No
(i.e. Were you satisfied that the person could understand the nature of the decision, why the decision needed to be made at the time and whether they could understand the likely effects of deciding one way or another or making no decision at all?)
Please give reasons:
b. At the date and time of this assessment, is the person able to retain the information long enough to use it to make the decision?
** None Yes No
(i.e. long enough to complete the decision-making process, including making and communicating their decision. Consideration should be given to the use of notebooks, photographs, videos, voice recorders, posters etc. to help the person record and retain the information)
Please give reasons:
c. At the date and time of this assessment, is the person able to use and weigh up this information as part of the decision-making process?
** None
(e.g. to consider the consequences, benefits and risks, of making the decision one way or another or making no decision at all? Understand the pros and cons)
Please give reasons:
d. At the date and time of this assessment, is the person able to communicate their decision?
** None Yes No
(Verbally, using sign language or by any other means?)
Please explain how the decision was communicated or give reasons if answer is ‘No’:
If the answer to any one of the four above questions is ‘NO’, is the inability to understand, retain weigh up or communicate caused by an impairment or a disturbance in the functioning of their mind or brain?
** None Yes No
Please give details. NB the impairment can be temporary or permanent and does not need to be a formal diagnosis.
Full name entered below will serve as my electronic signature, confirming that the information provided is accurate to the best of my knowledge.
Job Title
PART 3a Lasting Power of Attorney or Court Appointed Deputy
In cases where an individual lacks capacity, consent to share with family and friends on behalf of that person will need to be sought from any person holding lasting power of attorney (LPA) for the individual. A LPA must be approved and registered with the Office of the Public Guardian. Proof of this status will be required.
An individual may have a court-appointed deputy (CAD) to act for them. Evidence of the status of the CAD should be sought and the relevant court order produced.
A person holding either of these positions is entitled to make decisions about sharing the individual’s information with family and friends.
Where an individual does not have a LPA or CAD, then a best interests decision must be made, as set out in the Mental Capacity Act 2005. This decision must take into account any previously stated wishes of the individual regarding information sharing (made at a time they had capacity), and whether the loss of capacity is temporary or permanent.
Statement of consent to share information
Provide details of who the individual has consented to access their health and care information. Name/ Relationship/ Address and telephone number/ Notes (for example request for a specific piece of information to be withheld)
Full name entered below will serve as my electronic signature, confirming that the information provided is accurate to the best of my knowledge.
PART 3b: Best Interest Decision to Share Information with Family, Friends and Representatives:
If the individual lacks mental capacity and there is no-one with an LPA or a Deputy with the relevant authority (i.e. to make health and welfare decisions), a best interest decision must be made by the responsible professional.
The Mental Capacity Act 2005: http://www.legislation.gov.uk/ukpga/2005/9/contents requires the best interest decision maker to consult with family/friends/representatives (and/or advocacy service if appropriate) before making a best interest decision. However, as noted in the National Framework for NHS Continuing Healthcare and NHS-funded Nursing Care (see paragraph 92), “……The person leading the assessment is responsible for making this decision and should bear in mind the expectation that everyone who is potentially eligible for NHS Continuing Healthcare should have the opportunity to be considered for eligibility….”
Please give details of who has been consulted: (Include name, relationship, address and telephone number)
Please confirm who (family, friends, representatives) the information can be shared with: (Include name, relationship, address, telephone number and notes)
Is it in the Individual's best interests for information about their health and welfare to be shared for this purpose?
** None Yes No Non applicable
Reasons for decision:
Full name entered below will serve as my electronic signature, confirming that the information provided is accurate to the best of my knowledge.
Job title
If a request is received from anyone who is not the personal representative please find the links to the by guidance: Access to health and care records of deceased people here.
Part 4 - Consent to Share a Deceased Person’s Information
This section relates to retrospective checklists/assessments for NHS CHC undertaken after the individual has passed away.
Once a person has passed away, someone will be appointed to manage their affairs. This person will be the Personal Representative (PR) of the deceased.
Anyone designated with next of kin status does not have access rights to information relating to the deceased, unless they have permission from the PR.
The PR must provide two forms of ID (see Annexe A). The PR should also have an original version, or a certified copy, of one of the following documents, as proof of their PR status (the address of the PR should also be included in these documents):
a redacted copy of the will - showing who the Executor/Administrator is or
a sealed Grant of Probate (GoP) or a grant of letters of administration - which is confirmation the applicant is in the process of obtaining authority from the Probate Registry
Once a person has proved their PR status (as outlined above), they have the right to decide who the deceased’s information is shared with (and can change or amend that decision at any time).
Record document type
Record ID document type
Record Document Type
Record ID Document Type
Full name entered below will serve as my electronic signature, confirming that the information provided is accurate to the best of my knowledge.
Part 5: The below must be completed by the *Responsible Professional obtaining consent for information sharing with family, friends, and representatives:
Full name entered below will serve as my electronic signature, confirming that the information provided is accurate to the best of my knowledge.
Required
Annexe A - List of identity verification documents
Verification of identity:
To verify your identity, please provide a total of two documents:
one form of photographic personal identification and one document confirming your address
A full list of documents that can be used to verify your identity can be found on the gov.uk website.
Annexe B: NHSE CHC Consent Template Information Sheet - for Sharing:
This sets out the basis on which information is shared for the NHS CHC process.
NHS CHC and Information Governance:
NHS CHC Consent: The Legal Basis The Legal Basis to process data for NHS CHC is covered in UKGDPR in the following articles:
Article 6 – Public Task/Official Authority
“The processing is necessary for the performance of a task carried out in the public interest or in the exercise of official authority vested in the controller”
NHS CHC assessments are based on the NHS Commissioning Board and CCG Regulations 2012**, which create the official authority vested in the controller.
Article 9 – Provision of care and support to a person
“The processing is necessary for the purposes of medical diagnosis, the provision of health or social care or treatment or the management of health or social care systems and services......"
NHS CHC assessments can determine the provision of health and social care to a person and help manage health and care systems.
NHS CHC and Common Law Duty of Confidentiality (CLDC)Personal Data +Healthcare data =CLDC
Confidential Patient information is required for NHS CHC assessment, so CLDC needs satisfying.CLDC is satisfied on the basis that NHS CHC assessments are a statutory requirement (as laid out in the 2012 NHS Commissioning Board and CCG Regulations 2012**)
Sharing information with family, friends or a third sector representative or advocate, supporting the individual, is not covered by the NHS Commissioning Board and CCG Regulations 2012 **, so consent is required.
**The National Health Service Commissioning Board and Clinical Commissioning Groups (Responsibilities and Standing Rules) Regulations 2012 (legislation.gov.uk) (Refer to Part 6)
Patient Level Data Set (PLDS):
NHS England and Integrated Care Boards collect information about individuals who undergo the NHS CHC assessment process (including personal data), for the NHS CHC PLDS, to help achieve better patient outcomes, better experience, and better use of resources in NHS CHC.
The lawful basis for collecting this information is Article 6 (1) (c) of the GDPR enacted by the Data Protection Act 2018.
Please note that NHS CHC PLDS data is pseudonymised for analysis purposes.
Detailed information about the use of individual’s identifiable data is publicly available at
https://digital.nhs.uk/about-nhs-digital/our-work/keeping-patient-data-safe/gdpr/gdpr-register
For free, independent advice about NHS Continuing Healthcare please contact:
Beacon CHC | Free Information & Advice - Beacon CHC
National framework for NHS continuing healthcare and NHS-funded nursing care - GOV.UK (www.gov.uk)
Further Information can be recorded here (If required)